The landscape of cancer immunotherapy is undergoing a dramatic transformation. While immune checkpoint inhibitors targeting PD-1 and PD-L1 have revolutionized oncology, response rates remain limited to 20-40% of patients in most solid tumors. Similarly, anti-angiogenic therapies blocking VEGF have shown promise but face challenges with resistance and limited durability. The convergence of these two therapeutic strategies into single bispecific antibody molecules represents one of the most exciting developments in cancer drug development today, with over 16 pivotal clinical trials currently underway in non-small cell lung cancer (NSCLC) alone as of April 2026.
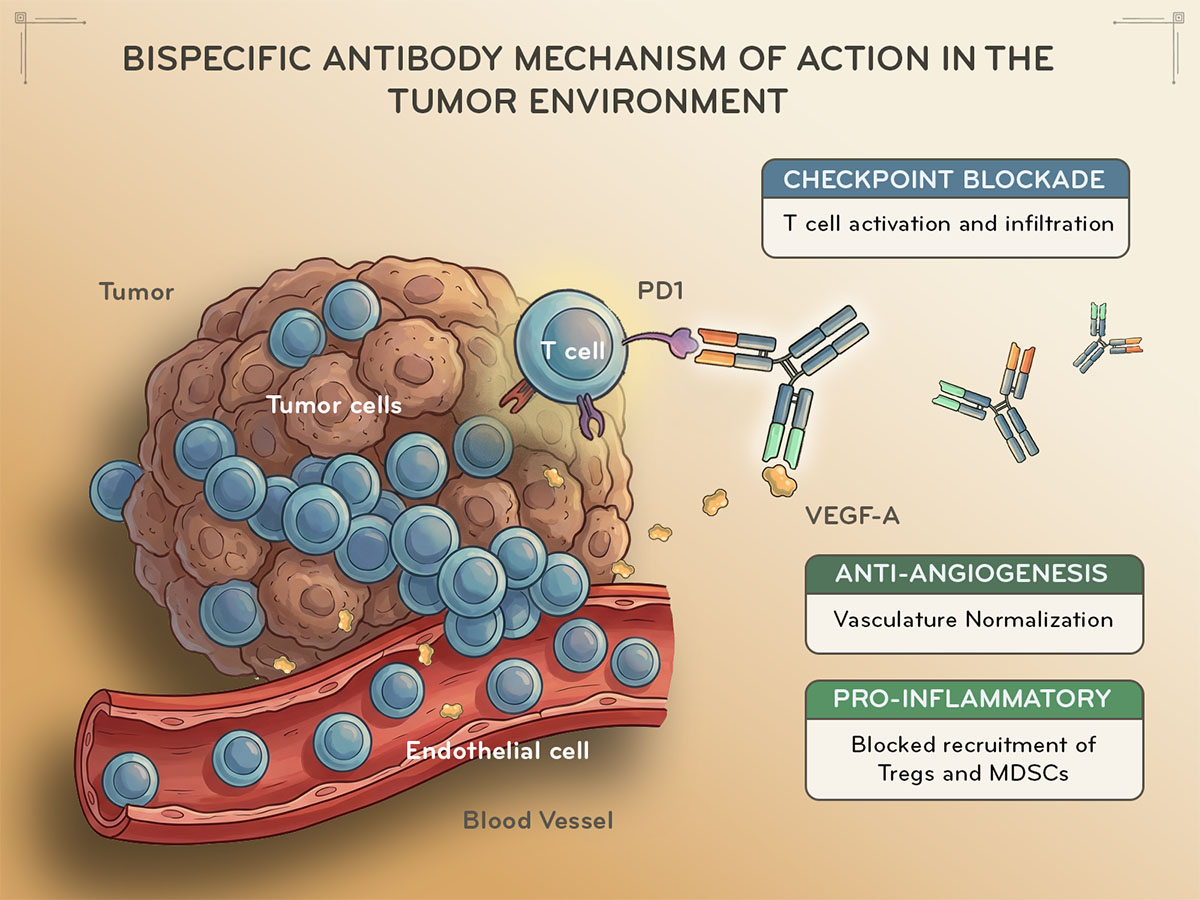
The combination of checkpoint inhibition and anti-angiogenesis is far from arbitrary—it's based on compelling biological synergy. VEGF, beyond its well-known role in promoting tumor blood vessel formation, actively suppresses anti-tumor immunity through multiple mechanisms. High VEGF levels in the tumor microenvironment recruit immunosuppressive cells including regulatory T cells (Tregs) and myeloid-derived suppressor cells (MDSCs), while simultaneously impairing dendritic cell maturation and T cell infiltration into tumors.
When VEGF is blocked, tumor vasculature undergoes "normalization"—abnormal, leaky vessels become more organized and functional. This normalization paradoxically improves the delivery and infiltration of effector T cells into the tumor core, precisely where PD-1/PD-L1 blockade can unleash their cytotoxic potential. Meanwhile, checkpoint inhibition removes the "brakes" on T cell activation, allowing these newly infiltrated immune cells to effectively attack cancer cells. This dual mechanism addresses two fundamental barriers to effective anti-tumor immunity: access (vascular) and activation (immune checkpoint).
PD-1/PD-L1 × VEGF bispecific antibodies are engineered to simultaneously bind immune checkpoint molecules and VEGF-A. The most common formats include IgG-scFv fusions, where a single-chain variable fragment (scFv) targeting one antigen is fused to a full IgG antibody targeting the other. This architecture ensures both activities are delivered to the same anatomical location with matched pharmacokinetics, resulting in a significant advantage over administering two separate monoclonal antibodies.
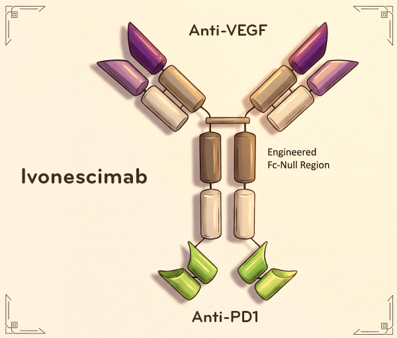
The clinical development of these bispecific antibodies has progressed with remarkable speed. Ivonescimab (AK112), developed by Akeso Biopharmaceuticals, has emerged as the frontrunner and is currently the only bispecific immunotherapy in Phase III trials for immune checkpoint inhibitor-resistant NSCLC. Phase II data presented at ASCO 2023 demonstrated promising anti-tumor activity when combined with chemotherapy, with a notably favorable safety profile showing no autoimmune-related adverse events, which is a significant concern with traditional checkpoint inhibitor combinations.
Other candidates are rapidly advancing through clinical development. Merck's MK-7684A showed encouraging Phase 1/2 data in Chinese NSCLC patients presented at AACR 2026, though the company remains cautious about Phase III commitments. IMM2510, representing the PD-L1 × VEGF approach, has demonstrated robust preclinical activity with dual binding confirmed and superior T cell activation compared to single agents in vitro.
The clinical landscape is expanding beyond NSCLC into colorectal cancer, gastric cancer, and hepatocellular carcinoma; tumor types where both angiogenesis and immune evasion play critical roles in disease progression.
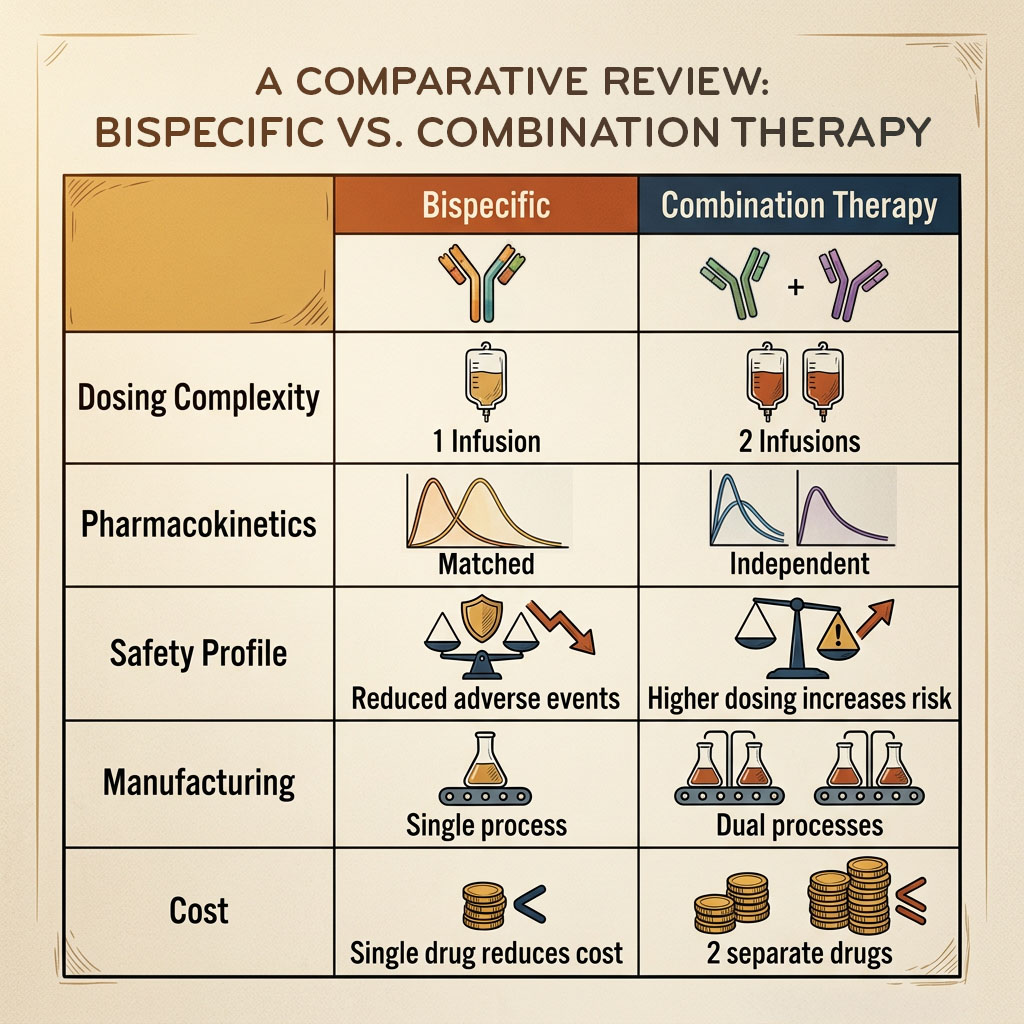
The bispecific approach offers several compelling advantages over administering separate anti-PD-1/PD-L1 and anti-VEGF antibodies. From a practical standpoint, patients receive a single infusion rather than two, reducing clinic time and improving compliance. Pharmacokinetically, the matched half-lives of both activities ensure synchronized pathway inhibition without drug- drug interaction concerns.
More importantly, the total antibody dose may be lower than combining two full-dose monoclonal antibodies, potentially reducing immune-related adverse events while maintaining efficacy. Early clinical data supports this hypothesis, with ivonescimab showing better tolerability than traditional checkpoint inhibitor combinations. The spatial co-localization of both activities at the tumor site may also enhance local efficacy through improved vascular normalization precisely where T cell infiltration is needed.
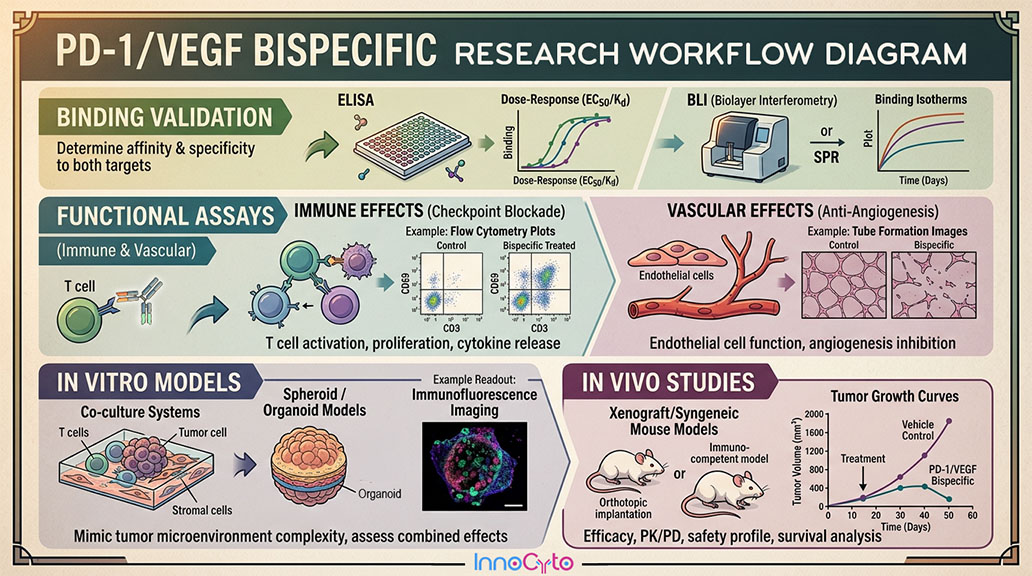
For researchers developing or studying these bispecific antibodies, several experimental systems are essential. Dual-target binding assays using flow cytometry or surface plasmon resonance confirm simultaneous engagement of both PD-1/PD-L1 and VEGF-A. Functional assays must assess both immune activation (T cell proliferation, cytokine production) and anti-angiogenic activity (endothelial cell proliferation, tube formation).
Advanced co-culture systems incorporating T cells, endothelial cells, and tumor cells in 3D formats provide physiologically relevant models for testing these agents. Biomarker studies require assessment of both PD-L1 expression and VEGF levels in the tumor microenvironment, along with vascular density (CD31 staining) and immune infiltrate characterization.
As we move through 2026, the field is poised for significant milestones. Phase III readouts for ivonescimab are anticipated, potentially leading to the first regulatory approvals for this drug class. The success of these agents is likely to spur development of next-generation formats, including trispecific antibodies incorporating a third target such as LAG-3 or TIGIT.
Biomarker-driven patient selection will become increasingly important, identifying which patients benefit most from dual checkpoint-angiogenesis inhibition versus other therapeutic strategies. The integration of these bispecifics into standard treatment algorithms, particularly in combination with chemotherapy or targeted therapies, will reshape cancer care across multiple tumor types.
PD-1/PD-L1 × VEGF bispecific antibodies represent a paradigm shift in cancer immunotherapy, elegantly addressing two fundamental mechanisms of tumor immune evasion in a single molecule. With robust clinical data emerging and multiple candidates advancing through late-stage development, this bispecific revolution is poised to deliver meaningful improvements in patient outcomes while simplifying treatment regimens. For researchers and clinicians alike, understanding the biology and clinical potential of these agents is essential as we enter a new era of precision immuno-oncology.
Contact us for expert support.